Surgical treatment on thoracolumbar burst fracture patients is to gain reduction and rigid fixation at the site of injury to gain persisting mechanical stabilization of the spine, achieve decompression of the nerves and restore nerve function.
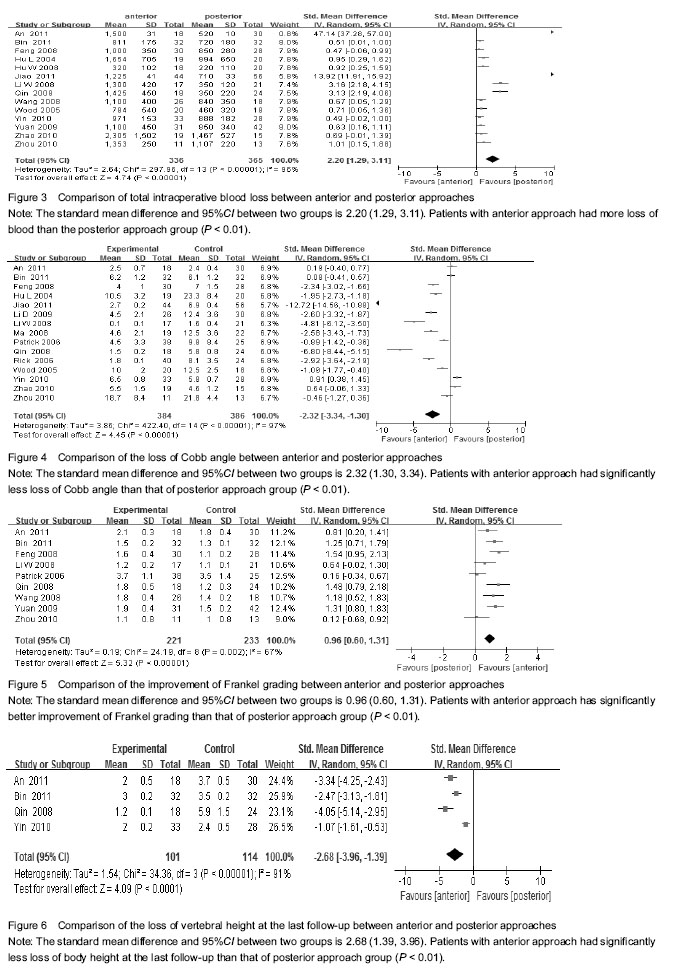
As the traditional way of surgery, posterior approach is an approach which is relatively simple and has small surgical trauma and little surgical complications. Analyzing from our meta-analysis, total time spent for the operation and hemorrhage during operation with the posterior approach were significantly less than that of the anterior approach.
Vertebral pedicle has the special anatomical structure of cortical bone surrounding the small amount of cancellous bone in the center. Posterior segment of the pedicle is composed of only cortical bone, which made it the strongest part in the vertebra, and pedicle screw fixation can enhance the stability of the vertebral body.
Posterior approach can recover the vertebral body height by stretching the posterior longitudinal ligament and the posterior fibrous ring and can achieve decompression of the canal by pushing back the bone block projecting into the spinal canal by the tension produced by the posterior longitudinal ligament. With the anterior pathway, on the other hand, internal fixation on the anterior and central pillar of the spine and intervertebral bone grafting can effectively restore the stress pathway of the spine and increases the fusion rate of the bone graft. Although pedicle screw fixation with posterior approach can reduce the bone block projecting into the spinal canal temporarily, supporting structure of bone trabecula in the vertebral body is not restored and doesn’t have weight bearing ability, which leads to loss of vertebral body height gradually. That may explain the result of the current meta-analysis that, loss of Cobb angle and vertebral body height at the last follow up is significantly higher with the posterior approach than the anterior approach. As the posterior approach may fail to construct the central pillar of the spine precisely, stress that was originally on the spinal column will concentrate on the internal fixation devise after the surgery, which leads to the break or loosening of the pedicle screw.
Moreover, posterior approach destroys the bony part of the posterior column, which decreases the spinal stability even further and leads to tardive kyphosis. Anterior approach can achieve thorough decompression and preserve the integrity of the posterior column. In the meanwhile, injured spinal column can be taken out and replaced by a bone graft to make sure that stable fusion at the injury site is achieved.
The current meta-analysis revealed that improvement in Frankel scores in the anterior approach group of patients is significantly better that of posterior approach group. Spinal cord injury after the thoracolumbar burst fracture is not only resulted from the primary violence, but also from the compression of anterior intervertebral disk tissue. Surgical decompression with posterior approach repositions the disk by stretching the anterior and posterior longitudinal ligament or gain indirect decompression by cutting off part of the lamina vertebra. This surgical procedure often results in the destruction of posterior longitudinal ligament, which leads to inadequate decompression of the spinal canal
[21]. Anterior reconstruction and internal fixation method makes it possible to remove what is compressing the spinal cord and avoids destroying spinal structures that play crucial role in protecting the stability of the spinal body. For similar reasons, anterior approach can also avoid stretching the dual sac and nerve root and iatrogenic injury to the spinal cord and facilitate the recovery of the nerve function after the spinal cord injury.
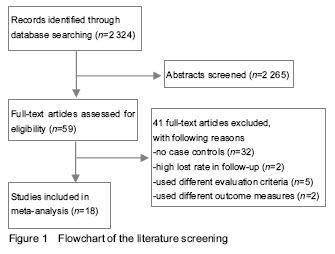
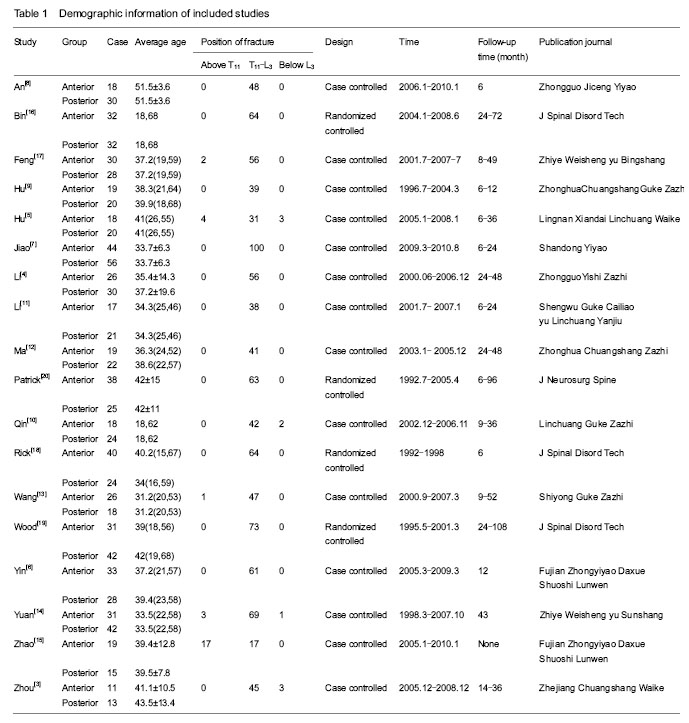
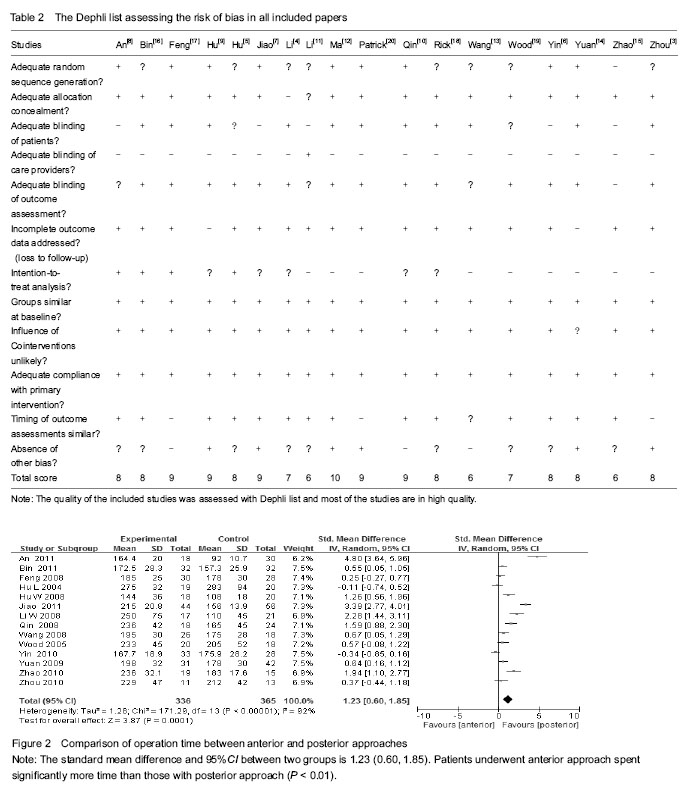
To our knowledge, the current meta-analysis is so far the study with the largest sample size. Although most of the studies included were published in Chinese language, the quality of those studies were tested by the Dephli list and proved to be qualified enough to be included in the meta-analysis.
CONCLUSION
Results of this meta-analysis reveals that although posterior approach for the surgical treatment of thoracolumbar burst fractures needs less operation time and has less blood loss, it is still inferior to anterior approach in respect of loss of Cobb angle, loss of the height of spinal body, improvement in Frankel and ASIA scores. Medical centers with adequate equipment and surgical technique can consider using anterior approach for the treatment of thoracolumbar burst fractures.